Did National Health Spending in 2020 Decline for the First Year in Recorded History? Preliminary Data Say It Did
February 16, 2021
On January 29, the US Bureau of Economic Analysis (BEA) released its initial estimate of December Personal Income and Outlays, allowing a preliminary look at national health spending for the entire year of 2020. Using our Health Sector Economic Indicators framework, we provide here an initial assessment of health spending and selected components in 2020, based largely on the latest BEA release.
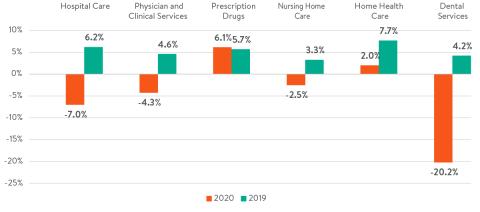
For the first year since at least 1960 – when the Centers for Medicare and Medicaid Services (CMS) began tracking national health expenditures – total health spending in 2020 was less than in the previous year. While spending has recovered somewhat from its pandemic-related decline in the spring, our preliminary estimate is that national health spending in 2020 was 2.0% lower than in 2019, a decline of about $75.8 billion dollars. The exhibit shows annual growth rates for six major personal health care components of health spending in 2020 and, for comparison, 2019. The latter numbers match the CMS National Health Expenditure Accounts (NHEA) for 2019, while the 2020 values are based primarily on the latest BEA data, adjusted to match more nearly those that would be produced by CMS.
Exhibit. Annual Health Spending Growth for Selected Categories, 2020 and 2019
Among the major contributors to the decline were hospital care, the largest component, which was 7.0% lower in 2020 than in 2019, and dental services, which dropped 20.2% in 2020. These declines and those in other categories occurred as some services were temporarily curtailed and patients avoided seeking care to avoid exposure to the COVID-19 virus. At the same time, spending on prescription drugs and home health care actually increased for the year, the latter likely related to individuals selecting home care rather than nursing homes to avoid exposure. Our recent Health Affairs Blog elaborates further on some of the probable reasons for the spending patterns observed in 2020.
The final CMS NHEA amounts for 2020 might differ from these preliminary numbers for two principal reasons: health spending in categories not tracked in the BEA data and the treatment of federal government financial support for the health sector. Our 2020 estimate is based largely personal consumption expenditures reported in BEA’s latest monthly release of the National Income and Product Accounts (NIPA), which provide detailed estimates of Personal Income and Outlays. Spending in some categories are not readily available in the NIPA, including services that are provided in non-traditional settings such as schools and workplaces, and categories that are not part of personal health care, including public health, research, investment in structures and equipment, and the net cost of private insurance. For these categories, which together made up 20.6% of national health expenditures in 2019, our estimates rely on the most recent CMS projections of national health expenditures. These projections were published last spring and do not reflect the impacts of COVID-19.
When these impacts are incorporated in the next annual update of the projections, our estimated 2020 change in national health spending will likely differ somewhat from the 2.0% decline that we currently estimate. The pandemic-induced recession may have suppressed spending on structures, equipment, and services provided in non-traditional settings to values below those in the projections. On the other hand, increased activity associated with COVID-19 testing, contact tracing, and early vaccination efforts might cause public health spending to exceed the projected values. Similarly, investment in COVID-related research could cause greater-than-projected spending within the research category. Finally, lower-than-expected spending on personal health care could result in lower medical loss ratios and a resultant higher value for the net cost of insurance than previously projected. Note that none of the above potential differences will impact the personal health care values shown in the exhibit, but they might cause our overall estimate of a 2.0% decline to be in error.
The second reason that our estimates might differ from the CMS NHEA values for 2020 relates to differences in the way BEA treats and CMS will treat payments from the federal government to hospitals and other health care providers in response to the recession, such as those mandated by the CARES Act. BEA treats these payments as grants or subsidies, while use of these funds to deliver health care is treated as consumption expenditures. Since our 2020 estimates for most personal health care expenditures rely on BEA’s tabulation of personal consumption expenditures, our estimates of spending growth will include these subsidies only when they have been applied to the delivery of health care. We understand that CMS is still investigating issues related to their treatment of these payments within the NHEA. However, expenditures reported by the NHEA are generally based on revenue received (including, for hospitals, non-patient revenue such as parking lot fees, gift shop sales, and grants). This could mean that our personal health care spending estimates understate the impact of these government payments to the extent that they are not used to provide patient care. (While our methodology adjusts for historical differences resulting from the differing methods used by BEA and CMS, it might not fully capture the impact of the large federal payments that are unique to 2020.) As a result, our estimates of the growth (or decline) in spending for the categories listed in the exhibit might be understated (overstated), compared with the ultimate NHEA values for 2020. Our estimates should, however, provide a reasonable characterization of the change in the level of care provided in 2020.
We will get a clearer picture of last year’s national health expenditures when the next CMS projections are released this spring and the 2020 historical data are published in December. While uncertainties currently exist regarding the final NHEA values, it is clear that health care goods and services delivered in 2020 declined from 2019.